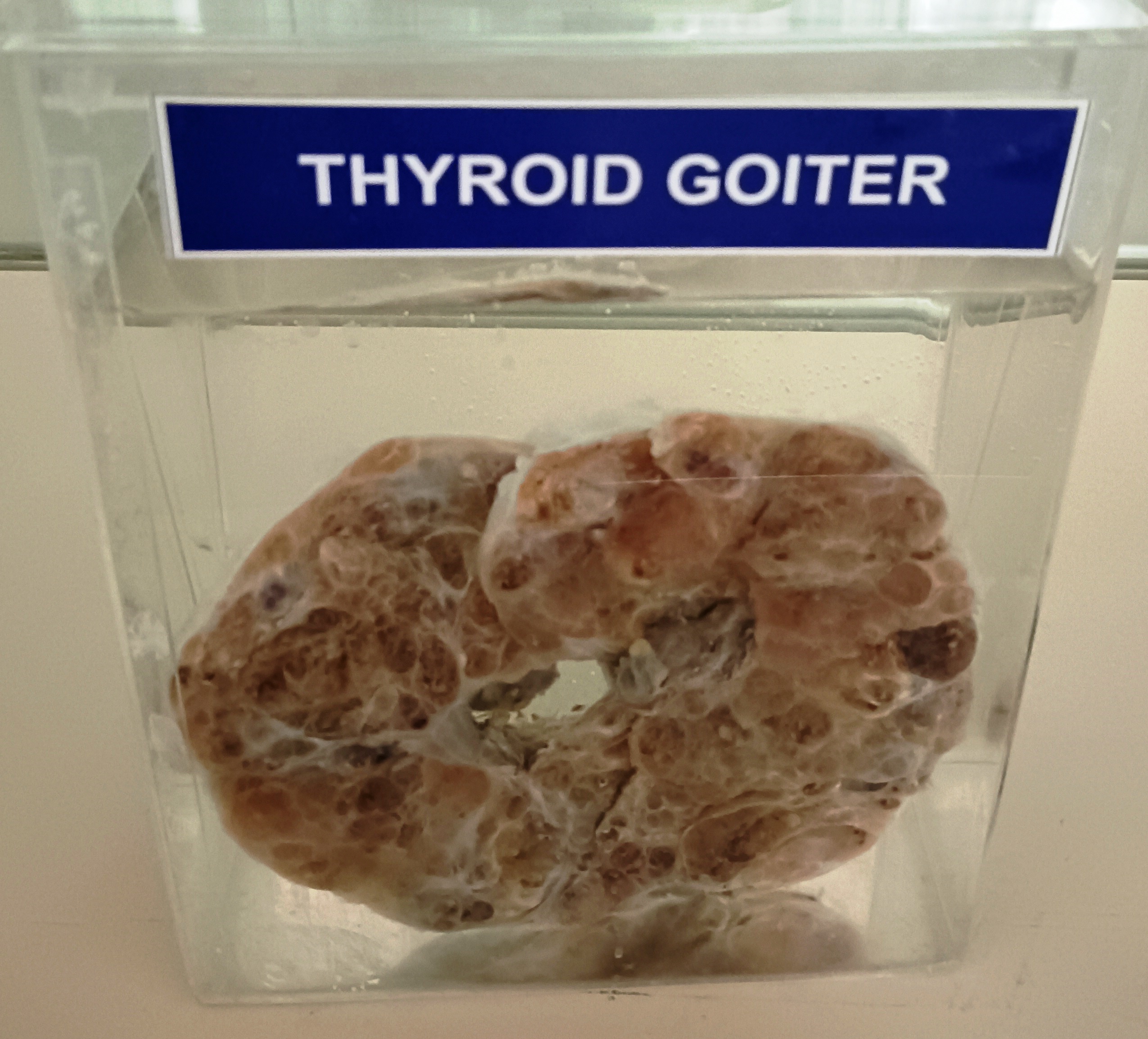
Thyroid goiter, also known as an enlarged thyroid gland, can have various pathological features. It is typically characterized by an increase in the size and weight of the thyroid gland, which can be caused by a variety of underlying conditions.
The most common pathological feature of thyroid goiter is a disruption in thyroid hormone synthesis, secretion, or metabolism, which can lead to the enlargement of the thyroid gland. This disruption can be caused by a variety of conditions, including iodine deficiency, autoimmune thyroid disease such as Hashimoto's thyroiditis or Graves' disease, and thyroid nodules or tumors.
In iodine-deficient goiter, there is a lack of iodine in the diet, which is necessary for the production of thyroid hormones. The thyroid gland compensates for the lack of iodine by enlarging in size, which can result in a diffuse or nodular goiter.
Autoimmune thyroid diseases such as Hashimoto's thyroiditis or Graves' disease can cause goiter through an immune-mediated attack on the thyroid gland. This can lead to inflammation and enlargement of the gland, which can be diffuse or nodular in appearance.
Thyroid nodules or tumors can also cause goiter, either by growing within the thyroid gland or by compressing the gland and causing it to enlarge. These nodules or tumors can be benign or malignant, and their treatment depends on their size, location, and pathology.
Pathological examination of thyroid goiter typically involves evaluation of the thyroid gland tissue for signs of inflammation, fibrosis, or neoplastic changes. Fine-needle aspiration biopsy (FNAB) is a common diagnostic tool used to evaluate thyroid nodules and tumors, which can help determine the nature of the nodule or tumor and guide appropriate treatment.