Specimen Image
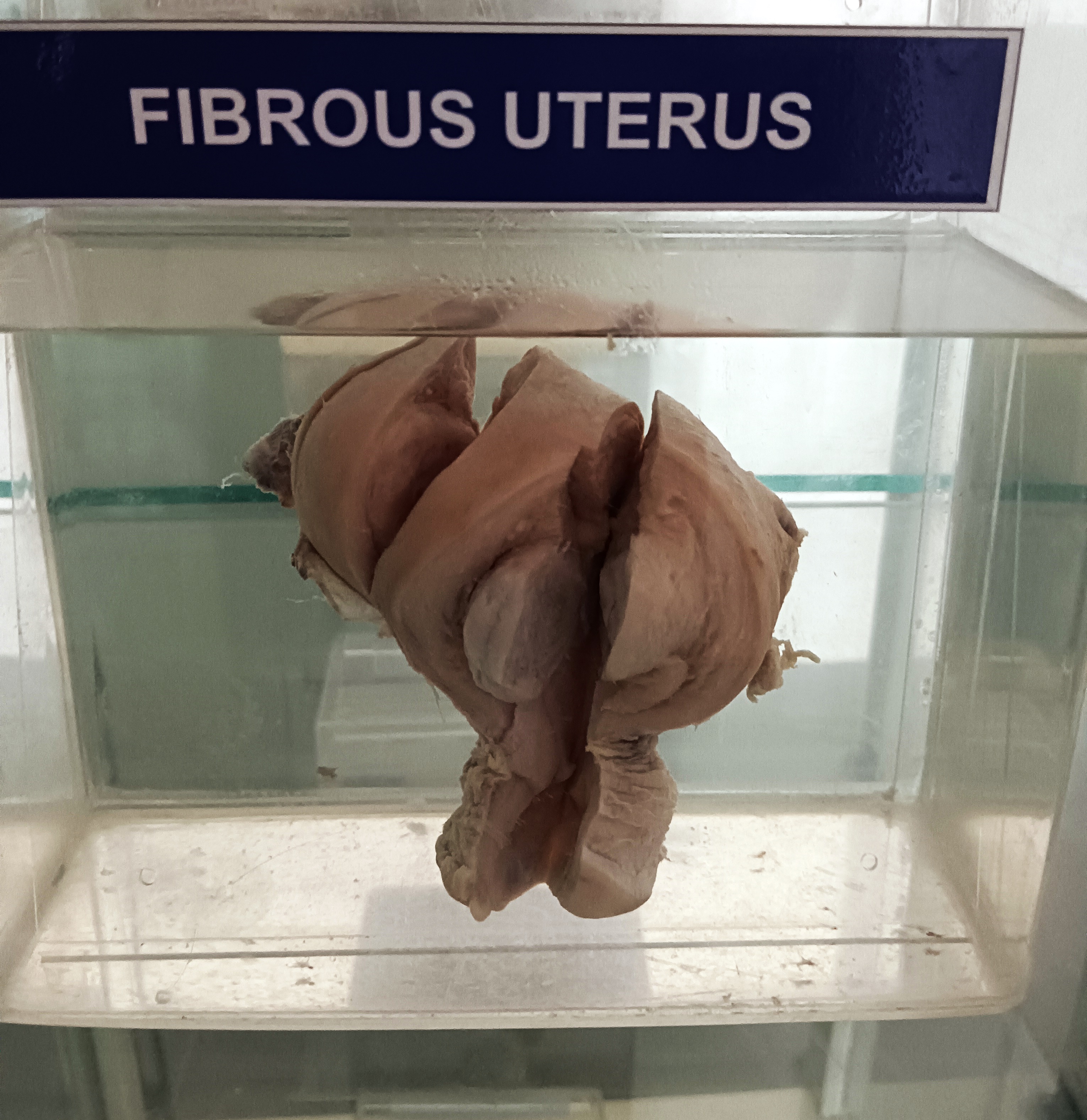
A fibrous uterus, also known as a fibroid uterus or uterine fibroids, is a condition where noncancerous tumors called fibroids grow in the muscle tissue of the uterus. The gross anatomy of a fibrous uterus can vary depending on the number, size, and location of the fibroids, but here are some general features:
- Enlargement of the uterus: The uterus may be larger than normal due to the presence of one or more fibroids. The fibroids can cause the uterus to grow in size and weight.
- Irregular shape: The uterus may have an irregular shape due to the presence of fibroids. The fibroids can cause the uterus to bulge in certain areas, making it appear irregular.
- Abnormal growths: The fibroids may appear as one or more masses or growths on the surface of the uterus. They may also be located inside the uterine wall or in the uterine cavity.
- Tissue changes: The tissue of the uterus may be firm and have a whorled appearance due to the presence of fibroids.
- Bleeding: Fibroids can cause heavy menstrual bleeding or prolonged periods. They can also cause bleeding between periods or after sex.
- Pressure symptoms: Fibroids can cause pressure on adjacent organs such as the bladder or rectum, leading to frequent urination or constipation.
Rack Number
Specimen Number
54